

Adhesive Capsulitis: What Causes Frozen Shoulder, and the Most Effective Treatment
Adhesive capsulitis is more commonly known as frozen shoulder because the condition involves a gradual “freezing” of the glenohumeral joint (shoulder joint). Over a period of weeks or months, the joint becomes painful and immobile. Initial onset to full recovery can take several years—but the good news is that with proper treatment, most people regain mobility and recover from this painful condition without surgery.
In this post, you’ll learn:
- What is a joint capsule?
- What is adhesive capsulitis (frozen shoulder)?
- The typical stages of frozen shoulder
- What causes frozen shoulder?
- What is the most effective treatment for frozen shoulder?
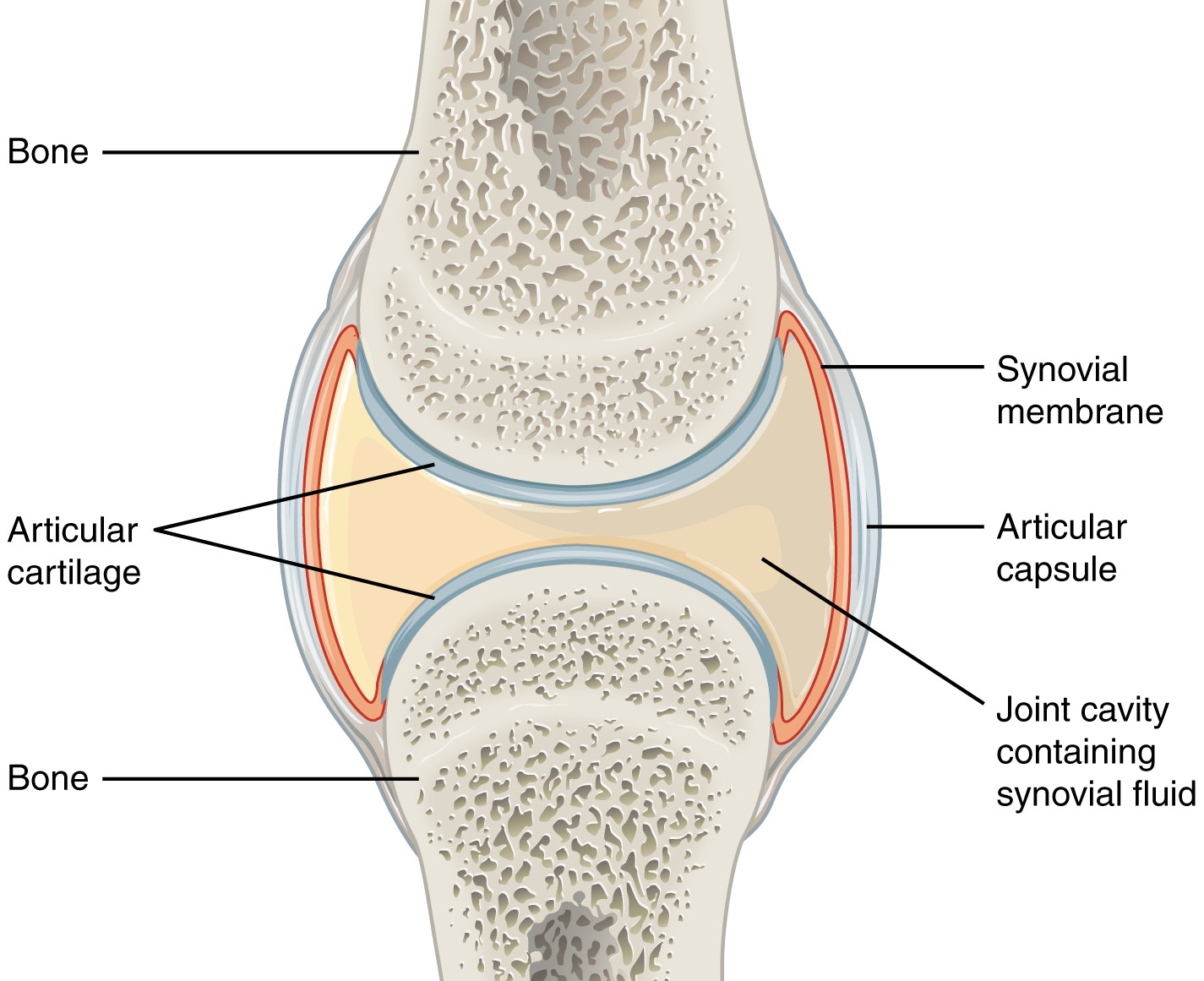
What is a joint capsule?
Every synovial joint in our body is protected by a joint capsule. The outer layer, the articular capsule, is made of dense connective tissue. Underneath the articular capsule lies the synovial membrane, which encases the synovial fluid; these three elements make up the joint capsule. Inside the capsule, cartilage protects the surfaces of the bones that articulate in the joint.
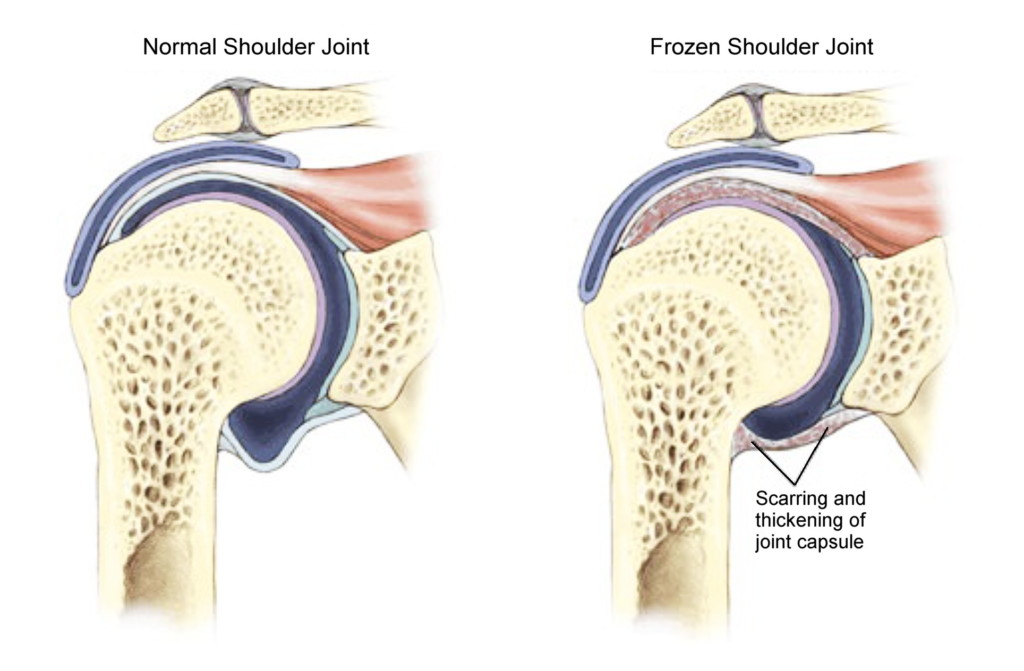
What is adhesive capsulitis?
In adhesive capsulitis (frozen shoulder), the joint capsule of the glenohumeral (shoulder) joint gradually becomes thicker and tighter, restricting movement and causing pain. There is a cycle of reduced mobility, inflammation, pain, formation of scar tissue, and tightening and thickening of the joint capsule that makes the condition continue to worsen. There can also be a decreased amount of synovial fluid present in the joint capsule, making movement more difficult. Abduction (moving the arm out and up to the side, away from the body) and external rotation tend to be particularly limited and painful.
Some conditions that have similar symptoms as frozen shoulder are: osteoarthritis, bursitis, tendinitis, rotator cuff pathologies, Parsonage Turner syndrome, a locked posterior dislocation, proximal humeral fracture, and active muscle guarding (chronically tight muscles).
The typical stages of frozen shoulder
Frozen shoulder typically progresses in three stages:
Stage 1: Referred to as the Acute, Freezing, or Painful Phase; typically lasts 6 weeks to 9 months. The shoulder joint is painful at the end of ranges of motion, and becomes painful at rest and overnight. Mobility of the joint gradually becomes limited.
Stage 2: Referred to as the Adhesive, Frozen, or Stiffening Phase; typically lasts 4 to 9 months. While pain may begin to subside, the joint continues to become more stiff and immobile.
Stage 3: Referred to as the Resolution, Thawing, or Recovery Phase; typically lasts 5 months to 3.5 years. Shoulder joint gradually regains normal mobility, and pain continues to subside.
What causes frozen shoulder?
Frozen shoulder is often directly related to lack of movement. It typically occurs in people who have had to keep their shoulder immobile after rotator cuff injury, a broken arm, or surgery, and people who have conditions that limit their mobility, like stroke or Parkinson’s disease. Reduced movement due to chronic tightness in the shoulder muscles likely contributes to idiopathic frozen shoulder, for which there is no obvious trigger.
Connective tissue adapts to the amount of movement demanded from it, becoming tighter with less movement and looser with more. This adaptation can lead to a vicious cycle: As the joint capsule gets tighter, movement becomes more difficult and sometimes painful, limiting movement further and causing the tissues to tighten even more.
Inflammation plays an important role in developing frozen shoulder as well. Following an injury or surgery, inflammation occurs in the joint as part of the healing process. This causes swelling, pain, and limited movement, and also causes scar tissue to form, making the joint capsule thicker and tighter.
Systemic inflammatory conditions, including diabetes and other metabolic conditions, osteoarthritis, thyroid disease, cardiovascular disease, and autoimmune diseases can also increase the risk of developing frozen shoulder.
What is the most effective treatment for frozen shoulder?
Gentle, natural movement has been shown to be the most effective treatment for frozen shoulder. A study of 77 patients with frozen shoulder compared the efficacy of intensive stretching and physical therapy to “supervised neglect,” defined as supportive therapy and exercises performed within a comfortable range of motion. Twenty-four months after the start of treatment, the supervised neglect group had regained 89% of their shoulder function, while the group receiving intensive stretching and physical therapy had only regained 63% of their shoulder function.
Another interesting study showed the role of chronic, involuntary muscle tension in frozen shoulder. Five patients who had been diagnosed with frozen shoulder underwent capsular release surgery to alleviate the contracture of their glenohumeral joint capsule. The patients’ range of motion was measured before and after being put under general anaesthesia. All five patients had significantly more range of motion of their shoulder joint when they were under anaesthesia; the increases in mobility ranged from 44˚ all the way up to 110˚. The researchers concluded that capsular contracture alone could not explain these patients’ loss of mobility, and that muscle stiffness or muscle guarding appears to be a major contributing factor to reduced range of motion in FS patients.
When we are in pain, we instinctively tighten up the muscles surrounding the painful area in order to limit movement and prevent further pain. So the presence of chronic muscle tightness in patients with frozen shoulder is not surprising; however, the substantial degree to which muscle tension limited these patients’ range of motion is significant. This finding, combined with the study showing the efficacy of supportive therapy and gentle exercises, points to Clinical Somatics exercises as being an ideal way to treat frozen shoulder. Moreover, since we know that the technique of pandiculation is the most effective way to release chronic, involuntary muscle contraction, Clinical Somatics could potentially allow patients to recover more quickly than with traditional methods.
If you have frozen shoulder and you want to use Clinical Somatics exercises to release your chronic muscle tension and improve your shoulder mobility, I recommend doing the online Level One & Two Courses. Below are the exercises from each course that will be most effective for you.
LEVEL ONE COURSE
Back Lift
Arch & Curl
Side Curl
One-sided Arch & Curl
Diagonal Arch & Curl
Washcloth
Carpal Tunnel Exercises
Flowering Arch & Curl
LEVEL TWO COURSE
Head Lifts
Scapula Scoops Part 1
Scapula Scoops Part 2
Proprioceptive Exercise 2
Diagonal Curl
Proprioceptive Exercise 3
Shoulder Directions
Shoulder, Elbow & Wrist Releases
Steeple Movement
Seated Twist
Proprioceptive Exercise 4
Recommended reading:
The Pain Relief Secret: How to Retrain Your Nervous System, Heal Your Body, and Overcome Chronic Pain by Sarah Warren, CSE
Somatics: Reawakening the Mind’s Control of Movement, Flexibility and Health by Thomas Hanna