

La cause de la scoliose idiopathique :
Contraction musculaire involontaire
La scoliose est considérée comme mystérieuse et incurable par de nombreuses personnes dans la communauté médicale. Alors que certains cas de scoliose sont causés par des anomalies structurelles congénitales ou des maladies neurologiques ou musculaires, la grande majorité (environ 85 %) est de cause inconnue.
The fact is, the bones in our body do not move unless our muscles move them. And our muscles are controlled by our nervous system. So when our vertebrae move out of alignment in any way, they are being moved by our muscles, which are being controlled by our nervous system.
Many cases of idiopathic scoliosis are caused by chronically tight muscles pulling the spine out of alignment. If you have idiopathic scoliosis, you can touch your back and waist and feel how tight your muscles are.
Si votre système nerveux envoie des messages à vos muscles pour qu'ils restent tendus, aucun allongement passif (comme des étirements statiques ou des massages) ou un réalignement forcé (comme un corset ou la chiropratique) ne modifiera ces messages.
In this post, we’ll talk about the patterns of muscular contraction that are common in idiopathic scoliosis, how our natural motor learning process leads us to develop these patterns, and how pandiculation retrains the nervous system to release chronic, involuntary muscular contraction.
“This is the best program I have encountered. I am a military veteran, with 2 tours to Afghanistan and have scoliosis which became much worse due to all the heavy lifting and carry overseas. These exercises have released the muscles and I am almost back to normal.”
-Alisa
Qu'est-ce que la scoliose ?
Scoliosis is a lateral curvature (side-bending) of the spine. A single curve in the spine is described as a C-curve. If the spine curves in both directions, it is described as an S-curve. If the degree of curvature is eleven degrees or more, it will be diagnosed as scoliosis.
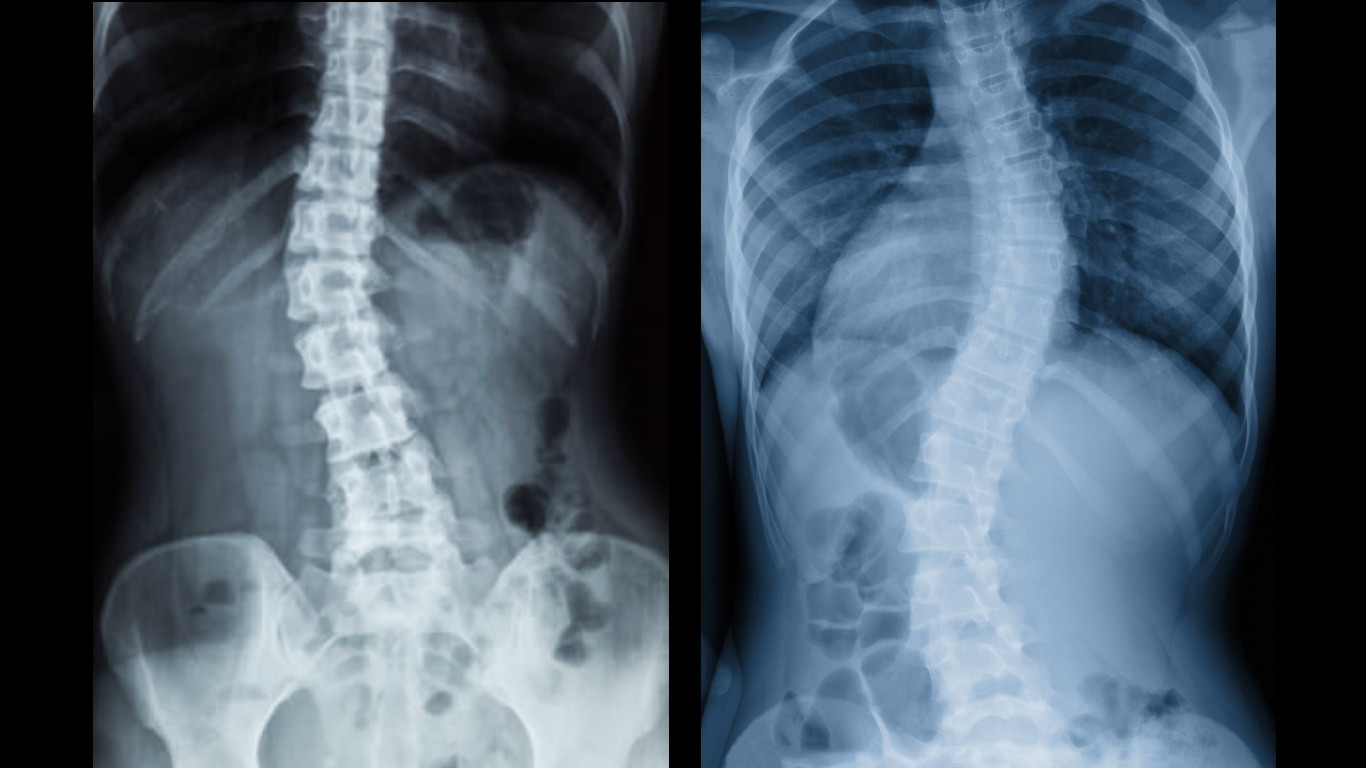
Gauche : courbe en C ; Droite : courbe en S
Types de scoliose
Approximately 85% of scoliosis cases are classified as idiopathic,1 which means that the cause of the spinal curvature is unknown.
In cases of congenital scoliosis, the spinal curvature is a structural abnormality that is present at birth.
In cases of neuromuscular scoliosis, the spinal curvature is caused by a neurological or muscular disease, such as cerebral palsy, spinal cord trauma, muscular dystrophy, spinal muscular atrophy, spina bifida, neurofibromatosis, or Marfan syndrome.
Les effets secondaires de la scoliose
Roughly two-thirds of adults with scoliotic curves between 20 and 55 degrees experience back pain.2 Many people with scoliosis develop pain in other parts of their bodies due to their postural misalignment, which puts uneven stress on the hips, knees, neck, and shoulders. Arthritis, disc and nerve compression in the spine, and difficulty breathing are also common.
Many people with untreated scoliosis, as well as some who have been surgically treated, develop spondylosis.2 Spondylosis is an arthritic condition of the spine in which joints become inflamed, cartilage thins, and bone spurs develop. Disc degeneration or spinal curvature can lead to spinal vertebrae pressing on nerves, resulting in severe pain and requiring surgery.
Le corset et la chirurgie sont-ils efficaces ?
Typically, bracing is recommended for curves greater than 25 degrees. Bracing attempts to slow or halt curve progression by forcibly aligning the spine. However, studies show mixed results when it comes to the efficacy of bracing,3 and some experts believe that the practice of bracing is outdated and ineffective. Patients who wear braces can also experience negative side effects such as pain, restricted breathing, and weakening or stiffening of their muscles due to lack of movement.
When curves progress to 45-50 degrees or more, spinal fusion surgery is considered. About 38,000 people undergo spinal fusion surgery each year in the United States.4 In spinal fusion surgery, metal rods, hooks, wires, and screws are attached to the spine in order to force it into a straight position. Then doctors attach pieces of bone, which grow together and create the actual fusion of the spine. Patients who undergo this type of surgery lose 20 to 60 percent of their spinal flexibility.5 A great deal of strain is put on the unfused parts of the spine, leading to a high rate of disc degeneration and osteoarthritis. Research shows that 75% of patients experience degeneration in their sacroiliac joints after spinal fusion surgery.6 And sadly, more than 40% of spinal fusion patients experience no reduction in their pain levels.5
Les taux de complications dans les chirurgies de fusion vertébrale varient, mais sont assez élevés dans tous les domaines. Certaines recherches ont montré que plus de la moitié des interventions chirurgicales échouent, ce qui signifie que les vertèbres ne fusionnent pas réellement. Même si les vertèbres sont maintenues en place par du matériel, les schémas de contraction des muscles du dos provoquent des micromouvements dans la colonne vertébrale, empêchant la croissance continue de l'os. La contraction musculaire peut être si forte que les tiges métalliques insérées le long de la colonne vertébrale se brisent, causant beaucoup de douleur et nécessitant une intervention chirurgicale répétée. Compte tenu du risque élevé de complications et du manque de preuves soutenant la fusion vertébrale en tant que traitement efficace, de nombreux médecins et chercheurs conviennent désormais que la chirurgie peut être utilisée pour ralentir ou arrêter la progression de la courbure, mais rien d'autre.
Les taux de scoliose idiopathique augmentent considérablement avec l'âge
A 2014 review published in American Family Physician found that approximately 85% of scoliosis cases are classified as idiopathic, or of unknown cause.1 So, 85% of the people who get diagnosed with scoliosis get no explanation as to what has caused it.
The same review found that between 2% and 4% of teenagers have scoliosis. According to a retrospective study done at Johns Hopkins University, the rate of scoliosis increases to more than 8% in adults over the age of 40.7 And a 2005 study of 75 healthy adults over the age of 60, with no previous diagnosis of scoliosis or spinal surgery, found the rate of scoliosis to be 68%.8
Cette prévalence croissante avec l'âge est un indicateur fort que la contraction musculaire due aux activités répétitives, aux blessures et au stress, dont les effets augmentent avec l'âge, joue un rôle dans le développement de la maladie.
Les schémas musculaires complexes impliqués dans la scoliose idiopathique
Notre colonne vertébrale peut fléchir (se plier) dans toutes les directions : vers l'avant, vers l'arrière et de chaque côté. Lorsque nous nous penchons dans n'importe quelle direction, nous pouvons également faire pivoter notre colonne vertébrale de chaque côté. Puisque nous avons 24 vertèbres articulées (en mouvement) dans notre colonne cervicale, thoracique et lombaire, et de nombreux muscles différents qui contrôlent le mouvement de nos vertèbres, nous pouvons développer des schémas variés et uniques de flexion et de rotation de la colonne vertébrale.
Scoliosis is never as simple as a single sideways bend or curve in the spine. We always compensate or balance ourselves out by developing other muscular patterns, like rotating to one side, arching our back, or rounding forward.
Parlons de certains des muscles les plus importants impliqués dans la scoliose :
The biggest, strongest muscles in our core that flex our spine laterally are our internal and external obliques. Our obliques also rotate our spine, so any chronic tension in our obliques will likely create both a lateral curve and some degree of rotation.
The erector spinae group of muscles travels from the base of the skull and cervical vertebrae all the way down to the pelvis, attaching to each vertebrae and rib. This group of muscles both laterally flexes the spine and extends it, meaning that it arches the back. So, chronic tension in these muscles can create both scoliosis and hyperlordosis, or an exaggerated arching of the lower back.
The intertransversarii are small, short muscles that connect each individual vertebrae to the vertebrae above and below it in the cervical and lumbar portions of the spine. These little muscles laterally flex the cervical and lumbar spine. Since they are the deepest muscles in the neck and lower back, they are nearly impossible to touch or sense internally.
We think of the quadratus lumborum (QL) as a lower back muscle, but technically, it’s our deepest abdominal muscle. The QL attaches our lowest rib to the top of our pelvis, and connects to our first through fourth lumbar vertebrae. This strong muscle laterally flexes our spine to either side, laterally tilts our pelvis (hikes our hips up one at a time), and helps to extend our spine. So, chronic tension in the QL not only contributes to lumbar scoliosis, but also to functional leg length discrepancy and hyperlordosis.
The latissimus dorsi is the broadest muscle of the back, spanning from the lumbar and lower half of the thoracic spine all the way to the upper arm just below the shoulder joint. The latissumus dorsi participates in many actions: extending, adducting, and medially rotating the shoulder, laterally flexing the spine, extending the spine, and even tilting the pelvis forward or to the side.
The transversospinalis group of muscles are small muscles in between each vertebrae, similar to the intertransversarii. But this group of muscles rotates and extends the spine, contributing to both scoliosis and hyperlordosis.
The most important thing to take away from this discussion is the fact that the muscular patterns involved in scoliosis can be very complex. All of the muscles in the core of the body, including some we haven’t mentioned, will be involved in the lateral flexion, rotation, and extension or forward flexion of the spine, as well as in the compensatory patterns we develop in order to balance ourselves out.
Le résultat de l'implication de tant de muscles multifonctionnels est que la scoliose idiopathique implique généralement une flexion latérale d'un ou des deux côtés, une rotation d'un ou des deux côtés, et une ou les deux extension et flexion vers l'avant. Ces virages et torsions peuvent se produire à différentes parties de la colonne vertébrale, créant des modèles de courbure vertébrale aussi uniques que nous.
Dans la section suivante, nous verrons comment et pourquoi nous développons ces schémas complexes de contraction musculaire.
And watch this video to learn how chronic muscle contraction pulls the spine into a curve.
Pourquoi nous développons la contraction musculaire involontaire qui cause la scoliose idiopathique
Comme je l'ai mentionné au début de l'article, nos os ne bougent que si nos muscles les font bouger. Et nos muscles sont contrôlés par notre système nerveux. Donc, si l'un des os de notre corps se désaligne, c'est parce que notre système nerveux envoie le message à nos muscles pour déplacer nos os de cette façon.
Pourquoi notre système nerveux enverrait-il le message de faire quelque chose qui pourrait nuire à notre corps ? Et pourquoi certaines personnes développent-elles une scoliose alors que d'autres non ?
The movement and level of contraction of our muscles is controlled by our nervous system. The way that our muscles move, and how much we keep them contracted, is actually learned over time by our nervous system.
Our nervous system learns certain ways of using our muscles based on how we choose to stand and move each and every day. Our nervous system notices the postures and movements that we tend to repeat, and it gradually makes these postures and movements automatic so that we don’t have to consciously think about them.
This learning process—that of developing what we refer to as muscle memory—allows us to go through the activities in our daily lives easily and efficiently. Unfortunately, if we tend to repeat unnatural postures or movements, our nervous system will learn those too. Our automatic neuromuscular learning process doesn’t discern what is good or bad for us—it just notices what we tend to repeat, and makes it automatic.
Donc, si vous portez votre sac du même côté tous les jours, tenez votre enfant sur la même hanche, asseyez-vous à votre bureau de la même manière ou adaptez votre posture à une blessure, les muscles qui fléchissent votre colonne vertébrale sur le côté peuvent facilement devenir chroniquement serré, conduisant à une scoliose idiopathique.
As your nervous system gradually learns to keep your muscles tight, gamma loop activity adapts. This feedback loop in your nervous system regulates the level of tension in your muscles. As your brain keeps sending the message to contract your muscles, gamma loop activity adapts and starts keeping your muscles tight all the time. Meanwhile, your proprioception (your internal sense of your posture and movement) adapts so that you’re not aware of the increased level of tension in your muscles or your altered posture.
De nombreuses personnes développent une contraction musculaire involontaire qui désaligne leur colonne vertébrale d'une manière ou d'une autre. la cyphose posturale (dos arrondi) et l'hyperlordose (bas du dos arqué) sont très fréquentes. La flexion latérale est également très courante, mais la courbure latérale de nombreuses personnes reste inférieure à 11 degrés tout au long de leur vie, de sorte qu'elles ne reçoivent pas de diagnostic de scoliose.
«Après avoir subi plusieurs blessures au corps, y compris une blessure au dos, ma colonne vertébrale courbée en S est devenue plus grave et douloureuse. J'ai essayé divers exercices, une thérapie physique et un cours de posture en ligne pour la scoliose. À moins d'avoir une chirurgie du dos, recommandée par un médecin orthopédique, rien n'a fonctionné.
I hit the jackpot with the Somatic Movement Center. After the first month of doing exercises in the Scoliosis Course, my back and sciatica pain are basically gone. The sciatica pain only flares up occasionally if I lift a heavy object or sit on a hard surface. If the pain persists, I immediately do one of the somatic exercises with fairly quick results. After three years of chiropractic treatment, I no longer need to continue my visits. Thank you, thank you, thank you, Sarah, for this gift that keeps on giving!”
-Roz
Soulager la scoliose idiopathique avec pandiculation
Alors, pouvez-vous relâcher la contraction musculaire involontaire, restaurer l'activité normale de la boucle gamma et recycler votre proprioception ? Oui, vous pouvez! La technique de mouvement de la pandiculation vous permet de faire toutes ces choses en envoyant des informations précises à votre système nerveux sur le niveau de tension de vos muscles.
Pandiculation releases subconsciously held muscular contraction and brings muscles back into voluntary control. Thomas Hanna incorporated the technique of pandiculation into his system of neuromuscular education called Clinical Somatic Education. Since this is already a long post, I’ll let you read more about pandiculation in this post.
La scoliose causée par des muscles tendus qui désalignent la colonne vertébrale est un problème fonctionnel. elle est causée par le fonctionnement du système nerveux. Tenter d'améliorer une courbe vertébrale fonctionnelle en utilisant une force manuelle, comme une attelle ou du matériel, est absurde et le plus souvent inefficace, car cela ne change pas les messages que votre système nerveux envoie à vos muscles pour rester tendus.
Likewise, manual therapy like chiropractic and massage does not change the messages that your brain is sending to your muscles. Changing these messages requires retraining your nervous system using active, conscious movement: namely, pandiculation.
Les patients atteints de scoliose idiopathique qui utilisent Somatiques Cliniques les exercices pour relâcher la contraction musculaire chronique qui cause leur courbure entraînent généralement une réduction ou une élimination de leur douleur ainsi qu'un redressement progressif de leur colonne vertébrale. Somatiques Cliniques les exercices sont très lents, doux et thérapeutiques, et conviennent à tous les âges et à tous les niveaux de forme physique.
For most people, idiopathic scoliosis does not have to be a life sentence. The earlier the condition can be addressed with neuromuscular education, the better. Years of pain and psychological suffering can be prevented with early, constructive intervention.
If you have idiopathic scoliosis and want to learn Clinical Somatics exercises at home, the best way to start is with Clinical Somatics for Scoliosis. This three-month online course teaches the exercises one-by-one through video demonstrationss, audio classes, and written explanations, and is an ideal way for beginners to learn the exercises at home.
“After doing the whole program of Sarah Warren’s – Clinical Somatics for Scoliosis and having read her book to understand exactly how somatics works, I managed to almost heal all my symptoms! My scoliosis unwinded and I can clearly see myself more elongated and almost straight in the mirror. Thank you Sarah. I am very glad I stumbled upon your website. Life saver.”
-Rawya Rotily
Voici quelques conseils généraux à suivre tout au long du cours :
Become very familiar with your pattern of curvature so that you know how to go about releasing the muscles that are causing it. Here is a simple example: If your curvature looks like this from behind (see image below), it means that the muscles on the right side of your torso are tight, creating the curve that is concave to the right.

Essayez de courber votre colonne vertébrale comme celle de l'image et vous sentirez les muscles du côté droit de votre taille se contracter.
As you learn the exercises, you should spend more time working with the muscles that are tighter. You can do more repetitions with your tighter side, and sometimes, you should try lying down and practicing the exercises only with your tighter side. When you stand up, you’ll feel unbalanced, but that’s part of the learning and adjustment process that your nervous system needs to go through. Be sure to do the Standing Awareness exercise before and after—this is a critical part of the process of adjusting your proprioception (your internal sense of your posture).
Au fur et à mesure que vous commencerez à relâcher vos muscles tendus et à ajuster votre posture, vous prendrez conscience des différents schémas de tension que vous avez de chaque côté de votre corps et vous comprendrez comment travailler avec chaque côté pour relâcher cette tension.
When you do practice the exercises on both sides, notice how each side of your body feels different. Are you using your muscles differently on each side? Can you sense your muscles more on one side than the other? Do you feel like you have more control on one side than the other? Is one side tighter or looser than the other?
You can then go back and forth from side to side, learning from your more coordinated side. If a movement feels easy or “right” on one side, try to replicate that feeling and way of moving on your other side.
Above all, be patient with yourself. Releasing the complex patterns of muscular tension that cause idiopathic scoliosis is like peeling an onion. You’ll discover many layers—many patterns of tension—along the way. It takes time for the nervous system and the tissues of the body to adjust to new ways of standing and moving, so don’t try to rush the process. The most important thing is that you’re heading in the right direction.
Prêt à commencer à apprendre ?
If you have idiopathic scoliosis and you want to learn Clinical Somatics exercises, the best place to start is Clinical Somatics for Scoliosis. This online course teaches the exercises through video demonstrations, audio classes, and written explanations, and is an ideal way for beginners to learn the exercises at home.
“I am 13 years old and recently diagnosed with right Thoracolumbar Idiopathic Scoliosis. My mum and I came across Somatic Movement Center sometime in August during the pandemic as we were looking for treatment options for my scoliosis. Based on how I was feeling and the fact that I was determined to get myself to a journey of healing, I began the course and for sure from the 1st day, I knew I was on the road to recovery. Never did I miss to do my daily course, I began feeling and experiencing a difference in my feeling. The course has made me feel amazing. Since the first time I tried it I felt a huge difference with my posture, pain and I felt soo relaxed that all my stress was gone. I have had such an amazing experience and I am grateful that I got to find Somatic Movement Center.
Thank you so much Sarah for this course. I feel more even and symmetrical and have been feeling even more relaxed, and whenever I feel pain I do the somatic exercises and it relieves all the pain I feel. I have even become more flexible and my muscles are not as tight as they were before. Thank you so much Sarah, you have no idea how much you have improved my quality of life and I am looking forward to continuing with Somatic Movement Center exercises to eventually aspire to have a normal spine again and more relaxed muscles.”
-Natasha Wanjiru
Les références
1. Horne, J.P., R. Flannery, and S. Usman. (2014) “Adolescent Idiopathic Scoliosis: Diagnosis and Management.” American Family Physician 89, no. 3: 193–198.
2. Shah, S.A., MD. “Scoliosis.”
https://www.nemours.org/content/dam/nemours/wwwv2/filebox/service/medical/spinescoliosis/scoliosisguide.pdf
3. Davies, E., Norvell, D., and Hermsmeyer, J. (mai 2011). “Efficacy of bracing versus observation in the treatment of idiopathic scoliosis.” Evidence-Based Spine-Care Journal; 2(2): 25–34. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3621850/
4. Information and Support. National Scoliosis Foundation. http://www.scoliosis.org/info.php
5. Weiss, H.R. and Goodall, D. (août 2008). “Rate of complications in scoliosis surgery – a systematic review of the Pub Med literature.” Scoliosis, 3, 9. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2525632/
6. Ha, K.Y., Lee, J.S., and Kim, K.W. (mai 2008). “Degeneration of sacroiliac joint after instrumented lumbar or lumbosacral fusion: a prospective cohort study over five-year follow-up.” Spine (Phila Pa 1976), 33(11):1192-8. https://www.ncbi.nlm.nih.gov/pubmed/18469692
7. Kebaish, K.M., et al. (avril 2011) “Scoliosis in Adults Aged Forty Years and Older: Prevalence and Relationship to Age, Race, and Gender.” Spine (Phila PA 1976) 36, no. 9:731–736.
8. Schwab, F. et al. (2005). “Adult scoliosis: prevalence, SF-36, and nutritional parameters in an elderly volunteer population.” Spine (Phila PA 1976), mai 1; 30(9):1082-5. https://www.ncbi.nlm.nih.gov/pubmed/15864163
Lecture recommandée:
The Pain Relief Secret: How to Retrain Your Nervous System, Heal Your Body, and Overcome Chronic Pain by Sarah Warren, CSE
Somatics: Reawakening the Mind’s Control of Movement, Flexibility and Health by Thomas Hanna